Fill Out a Valid Ri Accident Report Template
In Rhode Island, navigating the aftermath of a motor vehicle accident involves adhering to specific procedures mandated by the state, especially when it comes to reporting the incident. The State of Rhode Island and Providence Plantations Division of Motor Vehicles Accident Office has outlined a comprehensive process through the Motor Vehicle Accident Report form, located at 600 New London Avenue, Cranston, RI 02920-3024. This form must be completed using blue or black ink and it serves multiple crucial purposes, including the documentation of uninsured motorists, vehicle damage over $1000, property damage exceeding the same amount, and medical expenses resulting from injuries sustained in the accident. Additionally, it requires information about lost wages due to the accident, emphasizing the necessity for a detailed and accurate account of the event, the damage incurred, and the recovery process. The instructions for completing the form are straightforward, urging individuals to report factually and refrain from assumptions or guesses. Specifically designed sections on the form guide respondents through documenting their vehicle information, the other vehicle(s) involved, location and timing of the accident, as well as any non-vehicle property damage or personal injuries that occurred. Moreover, it requires a personal declaration under penalty of perjury, ensuring that all information provided is true to the best of the individual's knowledge. This document not only aids in the immediate assessment and rectification of damages but also serves a fundamental role in ongoing traffic safety and insurance processes in Rhode Island.
Ri Accident Report Preview
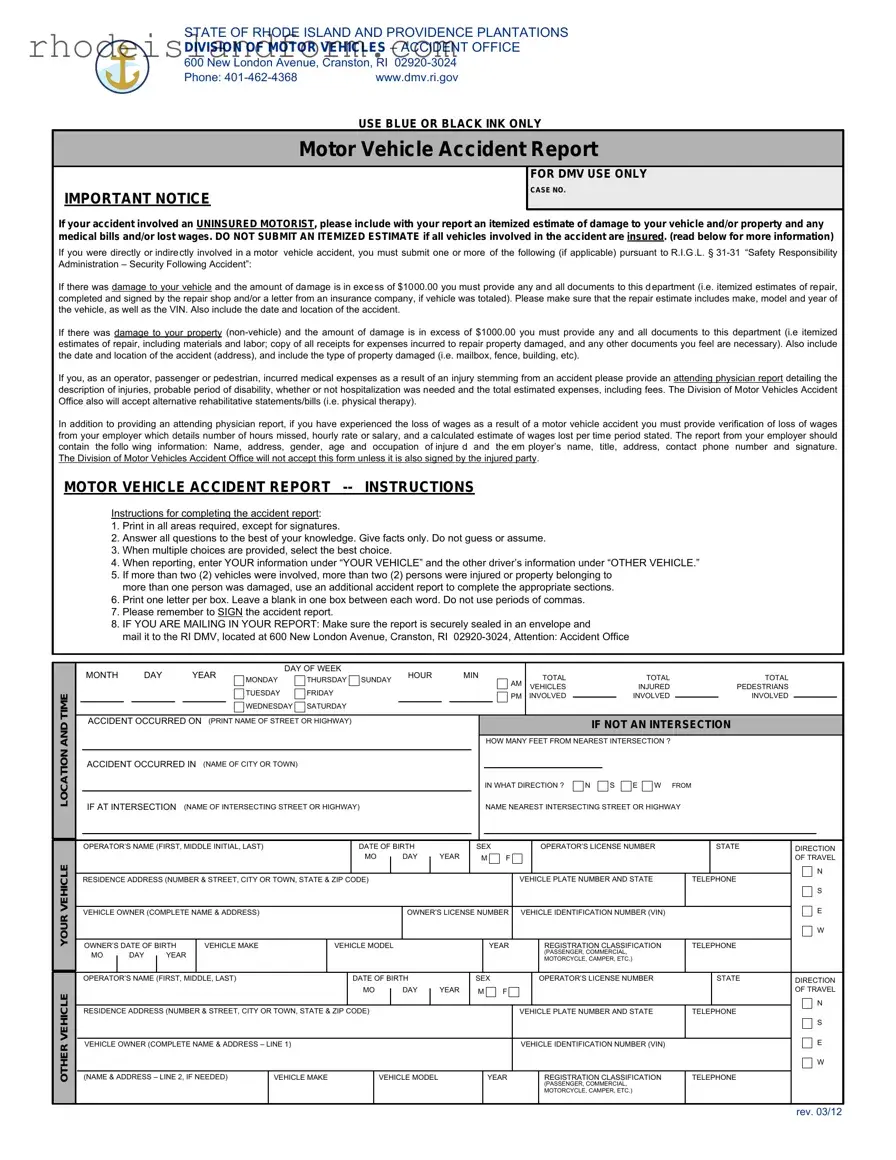
STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DIVISION OF MOTOR VEHICLES – ACCIDENT OFFICE
600 New London Avenue, Cranston, RI
Phone: |
www.dmv.ri.gov |
|
USE BLUE OR BLACK INK ONLY |
Motor Vehicle Accident Report
IMPORTANT NOTICE
FOR DMV USE ONLY
CASE NO.
If your accident involved an UNINSURED MOTORIST, please include with your report an itemized estimate of damage to your vehicle and/or property and any medical bills and/or lost wages. DO NOT SUBMIT AN ITEMIZED ESTIMATE if all vehicles involved in the accident are insured. (read below for more information)
If you were directly or indirectly involved in a motor vehicle accident, you must submit one or more of the following (if applicable) pursuant to R.I.G.L. §
If there was damage to your vehicle and the amount of damage is in excess of $1000.00 you must provide any and all documents to this department (i.e. itemized estimates of repair, completed and signed by the repair shop and/or a letter from an insurance company, if vehicle was totaled). Please make sure that the repair estimate includes make, model and year of the vehicle, as well as the VIN. Also include the date and location of the accident.
If there was damage to your property
If you, as an operator, passenger or pedestrian, incurred medical expenses as a result of an injury stemming from an accident please provide an attending physician report detailing the description of injuries, probable period of disability, whether or not hospitalization was needed and the total estimated expenses, including fees. The Division of Motor Vehicles Accident Office also will accept alternative rehabilitative statements/bills (i.e. physical therapy).
In addition to providing an attending physician report, if you have experienced the loss of wages as a result of a motor vehicle accident you must provide verification of loss of wages from your employer which details number of hours missed, hourly rate or salary, and a calculated estimate of wages lost per time period stated. The report from your employer should contain the follo wing information: Name, address, gender, age and occupation of injure d and the em ployer’s name, title, address, contact phone number and signature. The Division of Motor Vehicles Accident Office will not accept this form unless it is also signed by the injured party.
MOTOR VEHICLE ACCIDENT REPORT
OTHER VEHICLE YOUR VEHICLE LOCATION AND TIME
Instructions for completing the accident report:
1.Print in all areas required, except for signatures.
2.Answer all questions to the best of your knowledge. Give facts only. Do not guess or assume.
3.When multiple choices are provided, select the best choice.
4.When reporting, enter YOUR information under “YOUR VEHICLE” and the other driver’s information under “OTHER VEHICLE.”
5.If more than two (2) vehicles were involved, more than two (2) persons were injured or property belonging to more than one person was damaged, use an additional accident report to complete the appropriate sections.
6.Print one letter per box. Leave a blank in one box between each word. Do not use periods of commas.
7.Please remember to SIGN the accident report.
8.IF YOU ARE MAILING IN YOUR REPORT: Make sure the report is securely sealed in an envelope and
mail it to the RI DMV, located at 600 New London Avenue, Cranston, RI
|
|
MONTH |
|
DAY |
|
|
YEAR |
|
DAY OF WEEK |
|
|
|
HOUR |
|
|
|
MIN |
|
|
|
|
TOTAL |
|
|
|
|
TOTAL |
|
|
|
|
TOTAL |
|
|
|
|
||||||||||||||
|
|
|
|
|
MONDAY |
THURSDAY SUNDAY |
|
|
|
AM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
TUESDAY |
FRIDAY |
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLES |
|
|
|
|
INJURED |
|
|
|
|
PEDESTRIANS |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PM |
INVOLVED |
|
|
|
|
INVOLVED |
|
|
|
|
INVOLVED |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
WEDNESDAY |
SATURDAY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
ACCIDENT OCCURRED ON (PRINT NAME OF STREET OR HIGHWAY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IF NOT AN INTERSECTION |
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOW MANY FEET FROM NEAREST INTERSECTION ? |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
ACCIDENT OCCURRED IN |
(NAME OF CITY OR TOWN) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IN WHAT DIRECTION ? |
N |
|
S |
E |
W |
FROM |
|
|
|
|
||||||||||
|
|
IF AT INTERSECTION (NAME OF INTERSECTING STREET OR HIGHWAY) |
|
|
|
|
|
|
|
|
|
|
|
NAME NEAREST INTERSECTING STREET OR HIGHWAY |
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OPERATOR’S NAME (FIRST, MIDDLE INITIAL, LAST) |
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|
|
|
|
OPERATOR’S LICENSE NUMBER |
|
|
|
STATE |
|
DIRECTION |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
|
|
|
DAY |
|
|
YEAR |
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF TRAVEL |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
RESIDENCE ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE PLATE NUMBER AND STATE |
|
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
||||||||||||
|
|
VEHICLE OWNER (COMPLETE NAME & ADDRESS) |
|
|
|
|
|
|
|
|
OWNER’S LICENSE NUMBER |
VEHICLE IDENTIFICATION NUMBER (VIN) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
OWNER’S DATE OF BIRTH |
VEHICLE MAKE |
|
VEHICLE MODEL |
|
|
|
|
|
|
|
|
YEAR |
|
|
REGISTRATION CLASSIFICATION |
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
MO |
|
DAY |
|
YEAR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(PASSENGER, COMMERCIAL, |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTORCYCLE, CAMPER, ETC.) |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
OPERATOR’S NAME (FIRST, MIDDLE, LAST) |
|
|
|
|
|
DATE OF BIRTH |
|
|
|
|
SEX |
|
|
|
|
OPERATOR’S LICENSE NUMBER |
|
|
|
|
STATE |
|
DIRECTION |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MO |
|
|
|
DAY |
|
|
YEAR |
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OF TRAVEL |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
RESIDENCE ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE PLATE NUMBER AND STATE |
|
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
||||||||||||||
|
|
VEHICLE OWNER (COMPLETE NAME & ADDRESS – LINE 1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VEHICLE IDENTIFICATION NUMBER (VIN) |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
(NAME & ADDRESS – LINE 2, IF NEEDED) |
|
VEHICLE MAKE |
|
VEHICLE MODEL |
|
|
|
|
|
YEAR |
|
|
REGISTRATION CLASSIFICATION |
|
|
TELEPHONE |
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(PASSENGER, COMMERCIAL, |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTORCYCLE, CAMPER, ETC.) |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
rev. 03/12
STATE PROPERTY
CITY/TOWN PROPERTY
PRIVATE PROPERTY
OWNER’S NAME |
OWNER’S ADDRESS (NUMBER & STREET, CITY OR TOWN, STATE & ZIP CODE) |
HOME PHONE
CELL PHONE
WORK PHONE
DAMAGE DESCRIPTION
VEHICLE DAMAGE
APPROXIMATE COST TO REPAIR |
|
APPROXIMATE COST TO REPAIR |
|
YOUR VEHICLE (VEHICLE 1) |
$ ____________________ |
OTHER VEHICLE (VEHICLE 2) |
$ ____________________ |
INJURED
ACCIDENT CONDITIONS
|
|
|
|
|
|
|
|
NAME $1'$''5(66OF INJURED (FIRST, MIDDLE INITIAL, LAST) |
NUMBER & STREET |
CITY/TOWN |
STATE ZIP |
INJURED WAS RIDING |
|||
|
|
|
|
|
|||
|
|
|
|
|
IN VEHICLE # |
||
|
|
|
|
|
|
|
|
|
AGE |
SEX |
|
ACCIDENT SEVERITY CONDITION AT SCENE OF ACCIDENT |
|
PERSON INJURED |
|||||||
|
|
M |
F |
1 |
FATAL |
3 |
BRUISES OR ABRASIONS |
1 |
PEDESTRIAN |
5 |
VEHICLE OPERATOR |
||
|
|
|
|
2 |
PEDALCYCLIST |
6 |
VEHICLE PASSENGER |
||||||
|
|
|
|
2 |
BLEEDING OR BROKEN BONES |
4 |
COMPLAINT OF PAIN |
||||||
|
|
|
|
3 |
PASSENGER IN BUS |
7 |
MOTORCYCLE OPERATOR |
||||||
|
|
|
|
|
|
|
|
4 |
OTHER |
8 |
MOTORCYCLE PASSENGER |
||
NAME AND ADDRESS OF INJURED (FIRST, MIDDLE INITIAL, LAST)180%(5 |
675((7CITY/TOWN |
STATE=,3 |
|
INJURED WAS RIDING |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
IN VEHICLE # |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AGE |
SEX |
|
ACCIDENT SEVERITY CONDITION AT SCENE OF ACCIDENT |
|
PERSON INJURED |
|||||||
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
1 |
FATAL |
3 |
BRUISES OR ABRASIONS |
1 |
PEDESTRIAN |
5 |
VEHICLE OPERATOR |
||||||
|
|
|
|
2 |
PEDALCYCLIST |
6 |
VEHICLE PASSENGER |
||||||
|
|
|
|
2 |
BLEEDING OR BROKEN BONES |
4 |
COMPLAINT OF PAIN |
||||||
|
|
|
|
3 |
PASSENGER IN BUS |
7 |
MOTORCYCLE OPERATOR |
||||||
|
|
|
|
|
|
|
|
4 |
OTHER |
8 |
MOTORCYCLE PASSENGER |
||
ACCIDENT INVOLVED COLLISION WITH ...
1 |
PEDESTRIAN |
4 |
MOVING VEHICLE |
7 |
FIXED OBJECT |
10 OTHER _______________ |
2 |
PEDALCYCLE |
5 |
VEHICLE STOPPED IN ROAD |
8 |
OBJECT IN ROAD |
|
3 |
NO COLLISION – RAN OFF ROAD |
6 |
PARKED MOTOR VEHICLE |
9 |
NO COLLISION - OVERTURNED |
|
IN YOUR OWN WORDS, PLEASE DESCRIBE WHAT HAPPENED ...
I, THE UNDERSIGNED, DECLARE UNDER PENALTY OF PERJURY THAT ALL STATEMENTS MADE ON THIS REPORT ARE TRUE AND COMPLETE TO THE BEST OF MY KNOWLEDGE AND BELIEF.
OPERATOR’S SIGNATURE(THIS REPORT MUST BE SIGNED): |
PRINT YOUR NAME: |
|
|||||
|
|
|
|
|
|
|
|
YOUR INSURANCE |
|
INFORMATION |
WAS YOUR VEHICLE OR |
NAME OF YOUR INSURANCE COMPANY (NOT AGENT) |
POLICY NUMBER |
||
|
|
|
|
||||
|
THE VEHICLE YOU WERE |
|
|
|
|||
|
OPERATING INSURED |
|
|
|
|||
|
(LIABILITY INSURANCE) |
|
|
|
|||
|
AT THE TIME OF |
|
|
|
|||
|
THE ACCIDENT? |
|
|
|
|||
|
IF “YES”, COMPLETE |
NAME OF POLICYHOLDER |
STREET ADDRESS |
||||
|
ATTACHED FORM |
|
|
|
|||
|
YES |
NO |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
DATE: |
|
|
|
|
|
|
POLICY EFFECTIVE DATES |
|
|
|
FROM: __________________________ |
|
|
|
|
TO: _________________________ |
CITY/TOWN |
|
|
STATE/ZIP |
|
|||
YOUR MOTOR VEHICLE INSURANCE INFORMATION
DATE OF ACCIDENT: |
PLACE OF ACCIDENT: |
FOR DMV USE ONLY
CASE NO.
DESCRIPTION OF VEHICLE INVOLVED IN ACCIDENT MUST CORRESPOND TO “YOUR VEHICLE” ON ACCIDENT REPORT
VEHICLE MAKE: |
TYPE: |
YEAR: |
VIN: |
|
|
|
|
|
|
NAME OF OPERATOR: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF OWNER: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF INSURANCE COMPANY (NOT AGENT): |
|
POLICY NUMBER: |
EFFECTIVE PERIOD: |
|
|
|
|
FROM: ____________________ |
TO: ____________________ |
NAME OF POLICYHOLDER: |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
|
|
|
|
|
NAME OF INSURANCE AGENT |
STREET ADDRESS: |
|
CITY / TOWN: |
STATE / ZIP: |
WHO ISSUED POLICY: |
|
|
|
|
|
|
|
|
|
YOUR SIGNATURE: |
|
|
DATE SIGNED: |
|
|
|
|
|
|
FOR USE BY INSURANCE COMPANY ONLY - DO NOT WRITE IN THIS AREA
RETURN THIS FORM ONLY IF NO STANDARD POLICY WAS IN EFFECT AS ALLEGED BY MOTORIST
WITH REGARD TO AN AUTOMOBILE LIABILITY INSURANCE POLICY FOR THE POLICYHOLDER NAMED ON THE REVERSE SIDE HEREOF, THE UNDERSIGNED INSURANCE COMPANY ADVISED YOU IN ACCORDANCE WITH THE ITEMS CHECKED BELOW:
1 |
No policy was in effect on the date of the accident. |
|
2 |
Our policy for the named policyholder applies to him/her as the operator but it does not apply to the owner of the vehicle involved in the accident. |
|
3 |
Our policy applies to the owner of the vehicle, but does not apply to the operator of the vehicle involved in the accident. |
|
4 |
Our policy affords bodily injury coverage only. |
Remarks: |
|
|
|
5 |
Our policy affords property damage coverage only. |
|
To: STATE OF RHODE ISLAND AND PROVIDENCE PLANTATIONS DIVISION OF MOTOR VEHICLES
600 NEW LONDON AVENUE
CRANSTON, RI
DATE: _______________________________________
Name of Insurance Company
By:
Authorized Representative
File Breakdown
| Fact | Detail |
|---|---|
| Form Title | Rhode Island Motor Vehicle Accident Report |
| Location | Division of Motor Vehicles – Accident Office, 600 New London Avenue, Cranston, RI 02920-3024 |
| Contact Information | Phone: 401-462-4368; Website: www.dmv.ri.gov |
| Ink Requirement | Use blue or black ink only for completing the form |
| Reporting Requirement | Required for accidents involving uninsured motorists, damages over $1000, or personal injury |
| Governing Law | R.I.G.L. § 31-31 "Safety Responsibility Administration – Security Following Accident" |
| Document Submission | Submit itemized estimates, repair documents, medical bills, lost wages verification, and other pertinent documents if applicable |
| Form Instructions | Detailed guidelines provided for filling out each section correctly, including how to report multiple vehicles or injuries |
| Signature Requirement | The form must be signed by the injured party for it to be accepted |
| Insurance Information Section | Details of the insurance policy must be provided, including the policy number and period of coverage |
Ri Accident Report - Usage Guidelines
Filling out a Motor Vehicle Accident Report in Rhode Island requires attention to detail and the gathering of accurate information. This process is not just about documenting the incident for insurance claims but also fulfills legal obligations to report certain types of vehicle and property damage, as well as personal injuries, to the Division of Motor Vehicles (DMV). Accurate completion of this form ensures that all involved parties have their damages and injuries officially recorded, which can be crucial for receiving proper compensation and handling liability.
- Use only blue or black ink throughout the form to ensure clarity and legibility.
- Thoroughly read every section to answer questions accurately, providing facts without making assumptions.
- For sections providing multiple choice answers, select the option that best aligns with your situation.
- Enter your information in the section labeled "YOUR VEHICLE" and the other involved party's information in "OTHER VEHICLE."
- If the accident involved more than two vehicles, additional injuries beyond two persons, or property damage to items owned by more than one person, attach another accident report form to cover all necessary information.
- Within the provided boxes, print one letter or number per box, ensuring there is a blank box between each word. Avoid using punctuation such as periods or commas.
- Sign the form to affirm that all provided statements are true and complete to the best of your knowledge and belief. This is a mandatory step for the form's submission.
- When preparing to mail your report, place it in an envelope, seal it securely, and send it to the specified address: RI DMV, 600 New London Avenue, Cranston, RI 02920-3024, Attention: Accident Office.
By following these steps, you will have successfully completed the Rhode Island Motor Vehicle Accident Report form. This document is a critical piece of the post-accident process, helping to establish an official record of the incident. It’s important for all drivers to provide honest, accurate information to facilitate fair resolutions for all involved parties.
Essential Queries on Ri Accident Report
What information do I need to provide if I was involved in an accident with an uninsured motorist?
If your accident involved an uninsured motorist, you are required to include with your Accident Report an itemized estimate of damage to your vehicle and/or property. Additionally, if there were any medical bills or lost wages as a result of the accident, these should also be included with your report. Do not provide an itemized estimate if all vehicles involved in the accident are insured.
What prerequisites must be met for submitting a Motor Vehicle Accident Report to the RI DMV?
Following an accident, you must submit a Motor Vehicle Accident Report to the RI DMV if:
- There was damage to your vehicle and the amount of damage is in excess of $1000.00. All relevant documents, such as itemized estimates of repair or a letter from an insurance company if the vehicle was totaled, must be provided.
- There was damage to your property (non-vehicle) exceeding $1000.00. You should submit itemized estimates of repair, including materials and labor, along with copies of receipts for expenses incurred to repair the damaged property.
- You incurred medical expenses as a result of an injury from the accident. An attending physician report detailing your injuries, probable period of disability, hospitalization necessity, and total estimated expenses should be included.
- You experienced loss of wages due to the accident. Verification from your employer detailing hours missed and wages lost should be provided.
How do I complete the Motor Vehicle Accident Report form?
To accurately complete the Motor Vehicle Accident Report form, you should:
- Print in all areas as required, signatures being the exception.
- Answer all the questions to the best of your knowledge without guessing or assuming.
- Select the best choice when multiple choices are provided.
- Enter your information under "YOUR VEHICLE" and the other driver’s information under "OTHER VEHICLE."
- Use an additional accident report form if more than two (2) vehicles were involved, more than two (2) persons were injured, or if damage occurred to property belonging to more than one person.
- Print one letter per box and leave a blank box between each word. Do not use periods or commas.
- Ensure the form is signed before submission.
Where do I send my completed Motor Vehicle Accident Report?
Once you have completed your Motor Vehicle Accident Report, securely seal it in an envelope and mail it to the following address: RI DMV, 600 New London Avenue, Cranston, RI 02920-3024, Attention: Accident Office. Ensuring the report is fully completed and signed is essential for processing.
What happens if I do not submit a Motor Vehicle Accident Report following an accident?
Failure to submit a Motor Vehicle Accident Report, when required, could result in consequences under the law. The report assists in the assessment of damages and in determining any necessary actions following an accident. Without this report, you may face penalties or fines, and there could be a delay or denial in the processing of insurance claims related to the accident.
Common mistakes
Filling out the Rhode Island Accident Report form requires attention to detail and accuracy to ensure that the Division of Motor Vehicles has all the necessary information to process the report. However, common mistakes often made during this process can lead to delays or complications. Here are several mistakes to avoid:
- Not using blue or black ink: The form specifies that it should be completed using only blue or black ink. Using other colors can cause issues with readability and processing of the form.
- Incomplete information: Leaving sections of the form blank can cause significant delays. It's crucial to provide all requested information to the best of one's ability, as incomplete forms are not processed.
- Inaccurate details: It's important to ensure that all information on the form is accurate, especially vehicle and insurance information. Inaccuracies can lead to issues with insurance claims and further investigations.
- Failing to include documentation for uninsured motorists: If the accident involved an uninsured motorist, failing to include an itemized estimate of damage and any medical bills or lost wages can hinder the processing of the form.
- Incorrect or unclear accident description: The form requires a clear and factual description of the accident. Vague or incorrect descriptions can lead to misunderstandings about the events leading to the accident.
- Not signing the form: A common mistake is forgetting to sign the form before submission. An unsigned form is considered incomplete and will not be processed.
- Omitting additional necessary documents: Depending on the circumstances, such as property damage over $1000 or medical expenses, additional documentation must be attached. Failing to include these documents can lead to incomplete processing of the report.
- Improper mailing: If the form is not securely sealed in an envelope or sent to the wrong address, it may not reach the intended destination, leading to delays.
By avoiding these mistakes, individuals can ensure their Rhode Island Accident Report form is accepted and processed efficiently by the Division of Motor Vehicles. It is beneficial to thoroughly review the form and all attached documentation before submission.
Documents used along the form
Filing an accident report in Rhode Island often involves more than just completing the official form. It requires gathering and submitting additional documentation to offer a complete picture of the incident, its impact, and the financial toll it took on those involved. These documents are vital for insurance claims, legal processes, and personal records. Understanding each document's purpose ensures a smoother interaction with insurance companies, legal entities, and state departments.
- Police Report: An official record from law enforcement detailing the accident's circumstances, findings at the scene, and any citations issued. It serves as an authoritative account of the event.
- Insurance Policy Information: Documentation proving the existence and terms of the vehicle insurance policy at the accident time. It may include coverage limits and the policy effective dates.
- Medical Reports: Detailed accounts from medical professionals describing the injuries sustained, treatments proposed or administered, and the prognosis. These are crucial for claims involving bodily injuries.
- Photographs of the Accident Scene: Images capturing various angles of the accident site, vehicle damages, and any relevant road conditions or signage. They provide visual evidence supporting the accounts recorded in the accident report.
- Repair Estimates: Itemized estimates from auto repair shops detailing the cost of repairing the vehicle damage. These estimates must include parts and labor costs.
- Witness Statements: Written or recorded accounts from individuals who witnessed the accident, offering additional perspectives on how the incident occurred.
- Proof of Income Loss: Documentation from an employer verifying any loss of income due to injuries sustained in the accident. This typically includes the amount and period of income lost.
- Correspondence with Insurance Companies: All written communication between the involved parties and their insurance providers regarding the accident. This could include claim filings, updates, and settlement offers.
- Legal Documentation: If the accident led to legal action, any related court documents or correspondence with legal representatives would be pertinent. This includes lawsuits filed, court notices, and legal motions.
Accurately compiling and submitting these documents complements the Rhode Island Accident Report form, providing a comprehensive overview of the accident. It's a crucial step in ensuring that all parties involved – from insurance carriers to legal teams – have the necessary information to assess the event thoroughly. As such, keeping these documents organized and accessible streamlines the post-accident process, aiding in a more effective resolution of any claims or disputes.
Similar forms
The Ri Accident Report form is similar to several other types of documents used in different contexts, each serving to collect vital information after specific types of incidents or for specific processes. Understanding these similarities can help in comprehending the structure and purpose of the Ri Accident Report form.
The first document it resembles is the Insurance Claim Form. Both the Ri Accident Report form and an Insurance Claim Form collect detailed information about the parties involved, the extent of damage (whether to a vehicle or property), and descriptions of the incident. They require factual accuracy and completeness to ensure proper handling of the post-accident procedures. Insurance Claim Forms, like the Ri Accident Report, often ask for a detailed account of the incident, including date, time, and location, in addition to personal and insurance information of the involved parties.
Another similar document is the Police Incident Report. This form is used by law enforcement to officially document the details of an accident or a crime. Much like the Ri Accident Report, a Police Incident Report captures information about the time, location, and nature of the incident, details of the involved parties, descriptions of any damages or injuries, and a narrative account of what transpired. Both forms play crucial roles in the investigative and claims processes, serving as official records of the events.
The Workplace Accident Report also shares similarities with the Ri Accident Report. Typically used within an organizational context to report incidents that happen in the workplace, it collects information on the involved individuals, the circumstances of the accident, types of injuries or damages incurred, and initial estimates of losses. Similar to the Ri Accident Report, it is critical for initiating insurance claims, conducting investigations to prevent future incidents, and complying with health and safety regulations.
Despite the differing contexts—be it for insurance, law enforcement, or workplace safety—the fundamental purpose of these documents aligns with that of the Ri Accident Report form: to provide a structured method for reporting incidents, facilitating a clear and comprehensive account of events to support further action, whether it be for insurance claims, legal proceedings, or safety improvements.
Dos and Don'ts
When it comes to filling out the Rhode Island (RI) Accident Report Form, ensuring accuracy and completeness is crucial. The RI Division of Motor Vehicles relies on this documentation to understand the circumstances surrounding an accident. Here are several do's and don'ts that could guide you through the process of completing the form.
- Do use blue or black ink exclusively. This requirement helps maintain the legibility and official appearance of the document.
- Don't submit an itemized estimate if all vehicles involved in the accident are insured. This keeps the report focused on cases where uninsured motorists cause damage.
- Do provide detailed documentation for any damage to your vehicle or property that exceeds $1,000. This includes repair estimates, insurance letters, and any related receipts.
- Don't leave questions unanswered. Complete all sections of the form to the best of your knowledge, providing factual information without assumptions or guesses.
- Do remember to sign the accident report. An unsigned report might not be processed, delaying any potential claims or resolutions.
- Don't guess or estimate details when filling out the form. Accuracy is key in reporting the time, location, and specifics of the vehicles involved.
- Do mail your report securely to ensure it reaches the Division of Motor Vehicles without being tampered with or lost. This transmission of the document is as important as the information it contains.
Adhering to these do's and don'ts can streamline the process of reporting a motor vehicle accident in Rhode Island. By providing accurate and comprehensive data, you help the relevant authorities effectively manage the aftermath of traffic incidents. Remember, a well-documented accident report is not only a requirement but also a critical resource for addressing insurance claims and legal considerations.
Misconceptions
One common misconception is that you only need to file the RI Accident Report form if the police were called to the scene. In reality, Rhode Island law requires individuals involved in accidents with damages exceeding $1,000 or where anyone has been injured to file a report, irrespective of whether law enforcement was present.
Many believe that the accident report form is complicated and requires professional legal assistance to complete. While it's true that the form requires detailed information, it is designed to be completed by individuals directly involved in the incident. Guidance is provided within the document, making it accessible for most people to fill out on their own.
Another misconception is that the insurance company will handle the entire reporting process. Although insurers often require a copy of the accident report and may assist in its completion, the responsibility to submit the form to the Rhode Island Division of Motor Vehicles (DMV) Accident Office lies with the individual.
People often think the report must be filed immediately after the accident occurs. While it should be submitted promptly, Rhode Island law allows a reasonable period to gather necessary documents and information required for a complete and accurate report.
Some assume that the report is only for accidents involving two vehicles. However, the form must also be submitted for accidents involving pedestrians, cyclists, motorcyclists, and non-vehicle property damage, assuming the damage exceeds the stated threshold.
There's a misconception that you should only report accidents that occur in Rhode Island. If Rhode Island residents are involved in an accident out of state but deal with local insurance and consequences, they might still need to file a report, especially for insurance or legal purposes.
Many people believe that if their vehicle was not damaged, they do not need to file a report. However, if other property was damaged or if anyone was injured or claims to have been injured, a report is necessary.
It's commonly thought that you need to decide who was at fault before filing a report. The RI Accident Report form, however, is a factual account of what happened, not a determination of fault. Fault is determined later by insurance companies or through legal proceedings.
Some individuals are under the impression that filing an accident report will automatically increase their insurance premiums. Filing a report isn't a direct cause for an increase in insurance rates; rather, it's the determination of fault and the cost of claims that may affect premiums.
Finally, there is a misconception that personal injury claims can wait until fault is determined. If you were injured in the accident, it's crucial to file a report and begin the claims process promptly, as waiting could complicate claims and potentially exceed time limits for insurance or legal action.
Key takeaways
When completing the Rhode Island Motor Vehicle Accident Report form, it is crucial to use either blue or black ink to ensure the clarity and legibility of the information provided.
For accidents involving an uninsured motorist, the involved parties are required to submit an itemized estimate of damages and any relevant medical bills or lost wages. However, if all vehicles involved have insurance, submitting an itemized estimate is not necessary.
Documenting and reporting vehicle and property damage accurately is essential, especially when the estimated repair costs exceed $1000. This includes providing detailed repair estimates, letters from insurance companies if the vehicle was totaled, and receipts for property repair.
In cases where injuries occur, it is important to include an attending physician report with the accident report. This report should detail the nature of the injuries, the expected period of disability, hospitalization needs, and the estimated costs for medical care.
If the accident results in a loss of wages, verification from the employer detailing the loss is necessary. This documentation should include hours missed, rate of pay, and total estimated wage loss, alongside personal and employer information.
The form requires detailed information about the vehicles and individuals involved in the accident, including names, addresses, vehicle identification numbers (VINs), and insurance details.
It is essential to accurately describe the accident, including the location, time, and circumstances in the specified sections of the form. Providing a clear and factual account of the accident will aid in the processing of the report.
Signing the accident report form is mandatory. An unsigned form may not be accepted by the Division of Motor Vehicles Accident Office, and this could delay the resolution of any claims or legal matters associated with the accident.
Once completed, the report should be mailed securely to the Rhode Island Division of Motor Vehicles at the specified address. Ensuring the report is properly sealed and addressed helps in timely processing and reduces the chance of delays.
Discover Popular Templates
W9 I Can Fill Out Online - Its emphasis on accurate taxpayer identification promotes fairness in tax obligations, ultimately supporting the state's fiscal stability.
Rhode Island Tx 16 - Instructions on attaching the necessary W-2 forms for a Rhode Island Temporary Disability Insurance Tax refund claim.
Cm 010 - A tool for ensuring compliance with court rules from the commencement of a case.